
 When two people mention the same thing to me within a week, I know it’s time to take notice. This time it was 3-D mammograms (aka digital breast tomosynthesis). Hospital radiology departments and mammogram centers are marketing them as if they were the new female Viagra and yet. . . we don’t yet know if the risks are worth the benefits.
When two people mention the same thing to me within a week, I know it’s time to take notice. This time it was 3-D mammograms (aka digital breast tomosynthesis). Hospital radiology departments and mammogram centers are marketing them as if they were the new female Viagra and yet. . . we don’t yet know if the risks are worth the benefits.
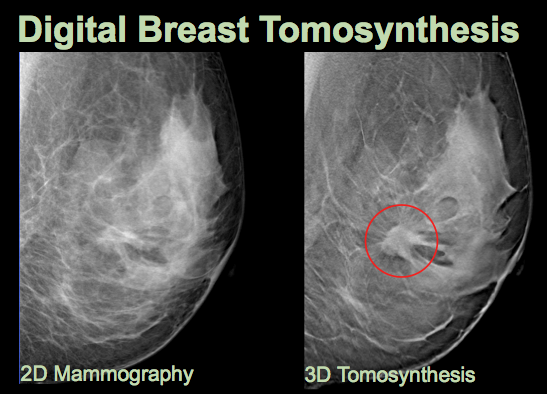
A traditional mammogram consists of vertical and horizontal images. The 3-D mammogram, as its name implies, provides a more holistic view as it swings in an arc around the breast, then combines those pictures into a three-dimensional image just like a CT scan. Studies find that combining the two may reduce call backs for additional tests and improve cancer detection rates. Overall, the National Cancer Institute reports, about 20 percent of breast cancers are missed during mammography and about 10 percent of women get called back for further screening.
I first heard about 3-D mammography during a dinner party, when a friend announced that she’d been diagnosed with early-stage breast cancer (actually, she’d been diagnosed with ductal carcinoma in situ [DCIS], which is not technically cancer). If it weren’t for this amazing new mammogram, she told us, her cancer might still be growing undetected. Then she proceeded to tell every woman at the table to make sure they opted for a 3-D mammogram. The 75-year-old woman sitting next me said she was going in for her mammogram the following week and absolutely would (never mind that current guidelines don’t recommend routine screening mammograms for women older than 74).
The problem is that there are risks associated with the technology (yes, Virginia, even mammograms can be risky). For instance, women still have to undergo the 2-D mammogram to get the 3-D mammogram, doubling their radiation exposure. We also don’t know which women are most likely to benefit from the 3-D screening, so for now it’s being sold to everyone.
A large study comparing the two for widespread screening found that of the 59 cancers found in 57 women, both mammograms found 39, but the combined 2-D/3-D found an additional 20. In addition, there were about half as many false positives in the combination. However, we don’t know if detecting those additional cancers reduced the risk of dying from the cancer, an important question required for any screening program. Plus, we have yet to see any large-scale, randomized controlled trials.
All of which is why insurance companies like Blue Cross/Blue Shield of North Carolina call the procedure “investigational” and refuse to pay for it, which means women have to fork over an extra $50 to $100.
Yet in an article in the local paper here touting the machines, the co-director of the regional breast center called 3-D mammogram “one of the biggest breakthroughs in mammography in the last 30 years.” Other words you hear bandied about are “state-of-the-art” and “groundbreaking.”
With language like that, what woman wouldn’t whip out her credit card?
That’s just what hospitals and imaging centers are relying on. At $700,000 per machine (plus annual service fees) they need to bring in a steady stream of breasts to cover their costs. Hence the massive, direct-to-consumer marketing.
It’s a bit like putting the cart before the horse. As the authors of an editorial on the topic wrote: “(Digital breast tomography) represents the most significant improvement in mammography development in recent years, if not decades, and shows extremely promising results in population screening. However, changing well-established
screening practice would be expected to have a major impact and should be based on strong and consistent evidence of benefit. Therefore, more evidence is needed from large-scale trials before a change in mammography screening practice can be recommended.”
Seems someone forgot to tell that to the mammography centers.